Introduction
The health outcomes associated with a
high salt diet are generally negative, and include increased risk of cardiovascular
disease risk, stroke, and kidney disease (1).
Because salt intake influences the total
osmolarity of your blood, increased consumption of salt, aka sodium-chloride (NaCl), rich
foods results in the body shunting more fluid to the blood, which requires
various compensatory mechanisms, including increased workload on the
cardiovascular system (2). There is substantial evidence that those at
risk for cardiovascular disease due to high blood pressure should reduce NaCl
intake. However, recent high impact
studies have been published that demonstrate salt intake may also influence the
progression of other diseases.
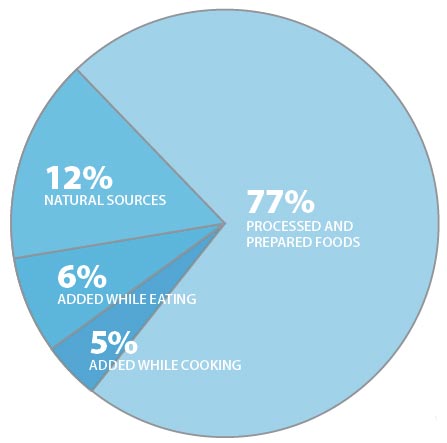 |
| Salt sources in American diet (source NIH) |
There has been a significant increase in the incidence and
frequency of autoimmune disease in the American population over the last half-century
(3). Examples of these diseases include
inflammatory bowel disease, rheumatoid arthritis, type I diabetes, multiple
sclerosis, and lupus erythematosis. In
order to understand whether certain environmental factors may be responsible
for the increased incidence of autoimmune disorders in the United States, researches have examined
the relationship between changes in the Western diet and immune function. Increased consumption of processed foods or “fast”
foods containing copious amounts of NaCl has represented a significant dietary
change over the past half-century (4), although the relationship
between high NaCl intake and autoimmune disease has not been well
characterized.
Cutting Edge
Recent studies published in Nature Letters have
provided a solid foundation for future research focused on the relationship
between NaCl intake and autoimmune immune disease. A recently discovered immune cell, known as a
Th17 T cell, has been suggested to play a role in the etiology of
numerous autoimmune and proinflammatory diseases. Th17 cells are known to heavily
participate in chronic inflammatory diseases as well as hyperactivation of the
immune system during immune responses to various pathogens such as influenza (5). Because these cells are mediators of
inflammation, they play a critical role in protecting the host from infectious
agents, however, excessive activation of the immune system resulting in chronic
inflammatory or hyperinflammatory responses has potentially lethal consequences
to the host.
Thus under normal circumstances, Th17 cells are
tightly regulated immune cells that are present at relatively low frequencies
in the body. In has been demonstrated
that Th17 cells can be found at increased numbers during autoimmune
disease, and deletion of Th17 cells using genetic ablation reduces
the severity of autoimmunity (5, 6).
These observations reinforce the notion
that Th17 cells are critical mediators of autoimmune disease. Because our understanding of these cells is in
its infancy, it is not quite understood what factors determine the production
of Th17 cells. However, among
various cytokines, the inflammatory cytokine, interleukin 23 (IL-23), has been
shown to stabilize and reinforce Th17 development (7).
In two very timely publications, scientists show that high
sodium (Na) plays a role in the development and pathogenic nature of Th17
cells. Studying the molecular aspects of Th17 cell differentiation, Wu et al. show high Na concentrations induce the
activation of signaling within T cells that supports development into Th17
cells (8). This was shown to be related to the activation
of an intracellular protein known as serum glucocorticoid kinase 1 (SGK1), a
salt-sensitive protein, meaning its activation is highly dependent on salt
concentrations. Activation of SGK1 in T
cells results in increased sensitivity to IL-23, which as mentioned earlier supports
Th17 development.

In the vary same issue of Nature Letters Kleinewietfeld
et al. discovered culture of human T cells in media containing increasing NaCl concentrations
promoted the development of Th17 cells in a dose dependent fashion (9). Using an “experimental” model of autoimmunity,
the authors of this study fed mice that were destined to develop autoimmune encephalitis
(an autoimmune disease similar to multiple sclerosis) a high salt diet and
found that mice fed a high NaCl diet presented with more severe autoimmunity
than mice fed a normal NaCl diet (9). Further studies by Wu et al. found that mice
fed a high salt diet alone had marked increase in the frequency of Th17
cells in gut associated lymphoid tissues, and that mice harboring a genetic
deletion of SGK1 had reduced Th17 cell development in response to a
high salt diet. Perhaps even more
important, Wu et al. present data in agreement with Kleinewietfeld et al. in
that mice fed a high salt diet exhibited more severe autoimmunity than mice fed
a normal salt diet and that this severe autoimmunity was SGK1 dependent.
Conclusions
Ok, great, but what does this all mean?
I’m sure the media will blow most of this out of proportion...
(Foxnews).
Do
these studies say that having a high salt intake will result in autoimmune
disease? NO.
These are experimental models of autoimmunity, in which mice
are immunized with proteins that forcefully induce autoimmunity. However, these two studies form an attractive
hypothesis supporting the role of the Western diet in immune dysfunction. Furthermore, these data provide
framework for future studies examining the direct role of NaCl intake on the
incidence of autoimmunity, especially in individuals who might be genetically
predisposed to developing autoimmune disease.
What can be taken away from these studies is that there is some
evidence that excess salt in the diet can alter immune cell development, which
has dangerous implications if one is predisposed to developing autoimmunity
(such as in these mice). The authors conclude
that determining whether a “true low-salt diet, representing the conditions in
which Homo sapiens were environmentally selected in Africa” has the
potential to reduce risk of autoimmunity will be very difficult because of
Western culture, which to me is a truly disappointing conclusion (obviously
they’ve never heard of Paleo!). Instead
the authors suggest looking for pharmacological agents that block the molecular
pathways described above (yay, just give people more drugs and lets continue to
eat like crap!). I think based on these
studies there is real evidence that high salt diets have the potential to
further exacerbate inflammatory responses which are clearly detrimental to
human health.
Works Cited
1. Brown IJ,
Tzoulaki I, Candeias V, Elliott P. Salt intakes around the world: implications
for public health. Int J Epidemiol. 2009 Jun;38:791-813.
2. Appel LJ,
Frohlich ED, Hall JE, Pearson TA, Sacco RL, Seals DR, Sacks FM, Smith SC, Jr.,
Vafiadis DK, Van Horn LV. The importance of population-wide sodium reduction as
a means to prevent cardiovascular disease and stroke: a call to action from the
American Heart Association. Circulation.
Mar 15;123:1138-43.
3. Ascherio A,
Munger KL. Environmental risk factors for multiple sclerosis. Part II:
Noninfectious factors. Ann Neurol. 2007 Jun;61:504-13.
4. McGuire S.
Institute of Medicine. 2010. Strategies to Reduce Sodium Intake in the United
States. Washington, DC: The National Academies Press. Adv Nutr. Nov;1:49-50.
5. Korn T,
Bettelli E, Oukka M, Kuchroo VK. IL-17 and Th17 Cells. Annu Rev Immunol.
2009;27:485-517.
6. Lee Y,
Awasthi A, Yosef N, Quintana FJ, Xiao S, Peters A, Wu C, Kleinewietfeld M,
Kunder S, et al. Induction and molecular signature of pathogenic TH17 cells.
Nat Immunol. Oct;13:991-9.
7. Aggarwal S,
Ghilardi N, Xie MH, de Sauvage FJ, Gurney AL. Interleukin-23 promotes a
distinct CD4 T cell activation state characterized by the production of
interleukin-17. J Biol Chem. 2003 Jan 17;278:1910-4.
8. Wu C, Yosef
N, Thalhamer T, Zhu C, Xiao S, Kishi Y, Regev A, Kuchroo VK. Induction of
pathogenic T17 cells by inducible salt-sensing kinase SGK1. Nature. Mar 6.
9. Kleinewietfeld
M, Manzel A, Titze J, Kvakan H, Yosef N, Linker RA, Muller DN, Hafler DA. Sodium
chloride drives autoimmune disease by the induction of pathogenic T17 cells.
Nature. Mar 6.













